 My dear friend emrcpian had recently posted a blog on abdominal examination and had mentioned about the use of 'traube's space'.
My dear friend emrcpian had recently posted a blog on abdominal examination and had mentioned about the use of 'traube's space'.It remains as elusive as it was back in my student years whereby conflicting opinions prevail till these days.
I had done some 'click and research' via the net. Would like to share :)
About Ludwig Traube, the original guru who described the Traube's space:
"Great merits and fame earned Ludwig Traube by establishing of the experimental pathophysiological research in Germany (e.g. he did animal experiments in the 1840th in his Berlin flat in the Oranienburger Str.) He improved the physical-medical methods like auscultation and percussion and was a taxonomist of the medical documentation. (e.g. inaugural of the temperature-pulse-frequenz of respiration-curve into clinical praxis). He investigated the pathophysiology of the respiration and the regulation of the body temperature, and gave a scientific basis to the digitalis therapy. The narrow coherencies between heart and kidney diseases have been well demonstrated. He worked together with Rudolf Virchow (1821-1902), they substantiated the „Beiträge zur experimentellen Pathologie“."
Wikipedia:
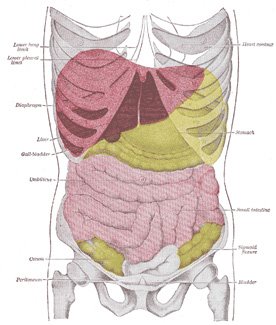
"Traube's (semilunar) space is an anatomic region of some clinical importance. It's a crescent-shaped space, encompassed by the lower edge of the left lung, the anterior border of the spleen, the left costal margin and the inferior margin of the left lobe of the liver. Thus, its surface markings are respectively the left sixth rib, the left anterior axillary line, and the left costal margin. Underneath lies the stomach, which produces a tympanic sound on percussion (medicine). If percussion over Traube's space produces a dull tone, this indicates splenomegaly. Assessing this may be more difficult in obese patients. The normal human spleen measures about 125mm in length, and splenomegaly is an important clinical sign. There are 2 possibilities to evaluate splenomegaly in the clinical examination: percussion and palpation. Percussion can be done in Traube's space, as described by his pupil in 1868. Another method was described by Donald O. Castell in 1967 (Castell's sign)."
Conclusion:
I think the percussion of Traube's space is both a non-sensitive and non-specific way of assessing for splenomegaly. As you can see, anatomically, it's bounded by the lower left lung, anterior border of the spleen and the left lobe of the liver. Hence theoretically, any enlargement/effusion of these structures could obliterate the space and hence would cause 'dullness' upon percussion.
As alluded earlier in Ludwig's biography, one of his main interests was in respiratory medicine. Hence it's not surprising that he had originally ascribed the dullness to pleural effusion instead :)
"Look out for the original papers decades back describing the eponymous syndromes or signs, and you'll be surprised how much they have evolved/changed through the years." -My neurology clinical mentor




